Alzhemier's Disease
Tanmatra and Alzhemier’s Disease

Ramesan Nair ,a character well depicted by
Mohanlal still remains in our hearts. Yes the same Ramesan Nair from the movie
" tanmatra" through whom we
came to know about the agony and hardships of the disease
"Alzheimers". It is a disease which cause a gradual loss of memory
with cognitive abilities. So in this blog i am
going to write about the Alzheimer's disease
Alzheimer’s Disease

Alzheimer's disease is a common neurodegenerative disease responsible for 60-80% of all dementias and imposing a significant burden on developed nations. It is the result of accumulation and deposition of cerebral amyloid-β (Aβ) and is the most common Cerebral amyloid deposition disease.
Epidemiology

Alzheimer disease is the
most common cause of dementia, responsible for 60-80% of all dementias .The
prevalence is strongly linked to age, with >1% of 60-64-year-old patients
being diagnosed with the condition, compared to 20-40% of those over 85-90
years of age .
Risk factors

Risk factors include:-
· Advanced age
· Female gender
· Current smoking
· Family history of dementia
· Mutations of amyloid precursor protein
· Down syndrome
· Chronic inflammation
In
addition to the genetic and environmental factors above, the age of
presentation is also influenced by socioeconomic factors
· Formal education
· Income
· Occupational status
· Social network and family support
Individuals with premorbid
higher function/supports are able to compensate for early disease changes to a
greater degree and thus present later. Consequently, when well-supported
patients eventually present, they tend to have more marked morphological
changes on imaging
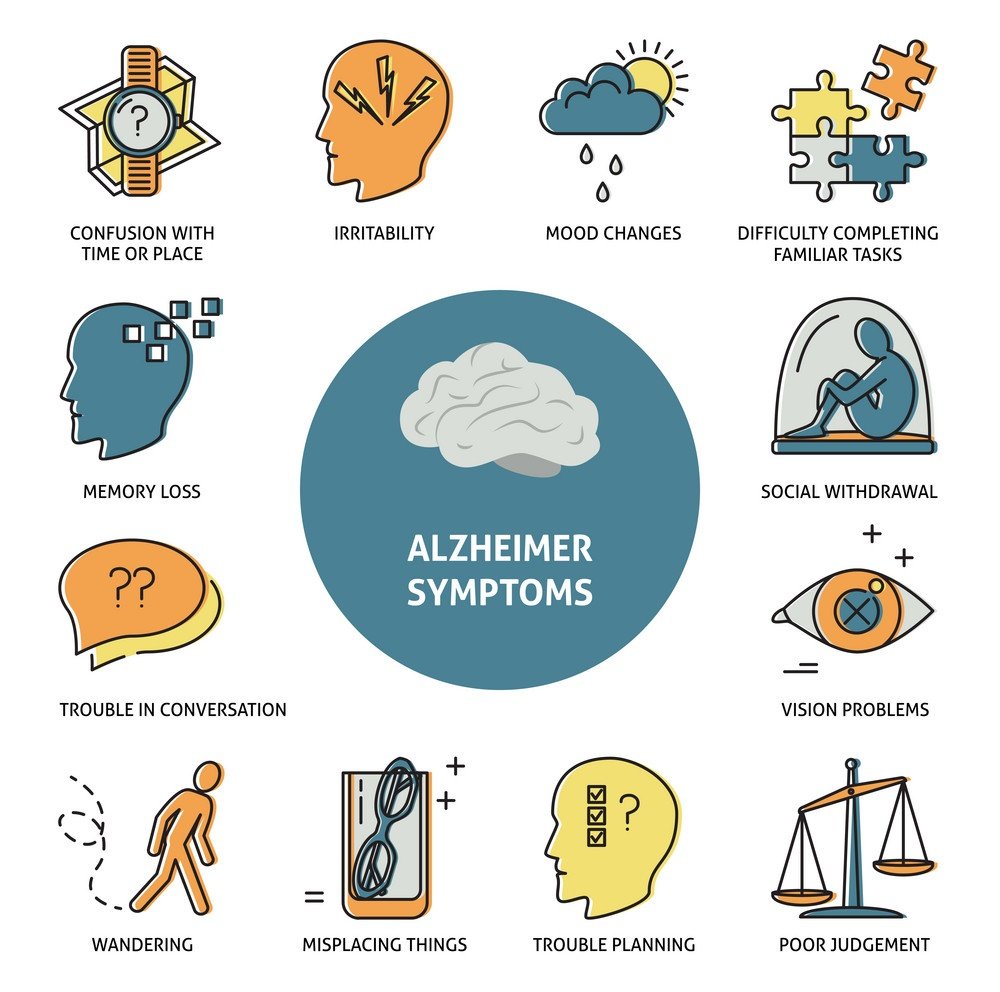
Clinical presentation
Traditionally, Alzheimer
disease has been clinically characterized predominantly by memory deficits, at
least in initial stages. It has become increasingly evident that in addition to
the typical presentation, a number of atypical clinical patterns exist, which
are nonetheless pathologically Alzheimer disease.

Classical/typical Alzheimer disease
The typical patient with
Alzheimer disease will present initially with antegrade episodic memory
deficits . Over time (often years), the disease progresses, with eventual
involvement of attentional and executive processes, semantic memory, praxis,
and visuoperceptual abilities. Neuropsychiatric symptoms are
also common and eventually affect almost all patients. These include apathy,
depression, anxiety, aggression/agitation, and psychosis(delusions and
hallucinations)
Atypical/variant Alzheimer disease
These entities, often
recognized clinically well before they were identified to be pathologically
identical to Alzheimer disease, are characterized by slowly progressive
focal cortical atrophy, with symptoms and signs matched to the affected area.
Examples include
·
Posterior cortical atrophy
·
Frontal variant of Alzheimer disease
·
Minority of cases with predominant semantic
dementia
Stages of Alzheimer's disease

1.Effect of aging on memory but not AD
· Forgetting things occasionally
· Misplacing items sometimes
· Minor short term memory loss
· Not remembering exact details
2.Early stage Alzheimer's
· Not remembering episodes of forgetfulness
· Forgets names of family or friends
· Changes may only be noticed by close friends or relatives
· Some confusion in situations outside the familiar
3.Middle stage Alzheimer's
· Greater difficulty remembering recently learned information
· Deepening confusion in many circumstances
· Problems with sleep
·Trouble determining their location
4.Late stage Alzheimer's
· Poor ability to think
· Problems speaking
· Repeats same conversations
· More abusive, anxious, or paranoid
Diagnosis
Clinical diagnosis is made
by identifying a progressive decline in memory both with clinical examinations
and neuropsychologic tests and has been historically based on the NINCDS-ADRA
criteria, which divides patients according to the certainty of the diagnosis
into:
1. Definite: clinical diagnosis and histologic confirmation
2. Probable: typical clinical syndrome without histologic
confirmation 81% sensitive, 73% specific
3. Possible: atypical clinical features without histologic
confirmation but no alternative diagnosis
Although using longitudinal
clinical criteria is highly sensitive in diagnosing a dementia of any type
(>90%), they are relatively inaccurate (<70%) in diagnosing Alzheimer
disease specifically.
Importantly, NINCDS-ADRA
criteria the only include imaging and laboratory examination or
blood and CSF in excluding other causes.
The only definitive
diagnostic test is brain biopsy which in practice is rarely obtained. As such,
the combination of clinical features and neuroimaging are usually considered
sufficient, although, especially with the recognition of variants, this
approach undoubtedly misdiagnoses a significant number of cases.
Pathology

Alzheimer disease is
characterized by the accumulation within the brain of cerebral amyloid-β
forming neuritic plaques,neurofibrillary tangles and eventually
progressive loss of neurons.
Cerebral amyloid-β
particularly deposits in association areas of the neocortex, the posterior
cingulate and precuneus, as well as the limbic cortex, although the reason for
this distribution has not been elucidated.
The underlying reason for
the accumulation of senile (neuritic) plaques and neurofibrillary tangles
remains poorly understood, as does the reason for non-uniform distribution in
the cortex.
There is, however,
increasing evidence to suggest that chronic inflammation is at least partially
responsible. Such inflammation can lead to prolonged parenchymal activation of
microglial cells which in turn results in the release of inflammatory mediators
with subsequent neuronal damage and amyloid-induced neurodegeneration.
Treatment and prognosis

· There is no cure for this disease; some drugs have been developed trying to improve symptoms or, at least, temporarily slow down their progression.
· Cholinesterase inhibitors e.g. donepezil
· Partial NMDA receptor antagonists
· Medications for behavioral symptoms
1. Antidepressants
2. Anxiolytics
3. Antiparkinsonian (movement symptoms)
4. Anticonvulsants/sedatives (behavioral)
Conclusion
Alzheimer’s is a family disease…it requires countless hours of care, which are typically provided by family caregivers…without professional help,it can be impossible to juggle providing that care with jobs,raising kids or just time for yourself



👍👍👍
ReplyDeleteThank u
DeleteThank u
DeleteGood work😁
ReplyDeleteThank u..
Delete